John A. Hodges, DDS, FICOI, says, “After the recent denial of full-arch rehabilitation for a patient of mine, I decided to try a different approach with her medical insurance company. I posed this question: Regardless of their policy toward dental implant coverage, in this patient’s case would they be financially better off paying to treat her with fixed implant-supported bridges versus not doing so and then having to pay for the future digestive complications associated with a failed oral system?
The act of chewing efficiently has a significant impact on a person’s digestive process. Proper and efficient chewing not only reduces the food particle size to aid in digestion and nutrient extraction, but increased saliva secretion from chewing lubricates food particles for easier and safer swallowing. Salivary enzymes initiate the breakdown of carbohydrates and fats, and increased saliva production signals the brain to tell the stomach to produce acids, the pancreas to secrete digestive enzymes, and the small intestine to prepare for absorption.
When a person chews at or near maximum chewing efficiency he or she is able to greatly increase the surface area of the food bolus, which assists the body in the extraction of nutrients. (1) At the Institute of Food Technologists’ Annual Meeting in 2013, Purdue University presented the results from a study that researched food absorption. Researchers concluded, “Particle size affects the bio-accessibility of the energy of the food that is consumed. The more you chew, the less is lost and the more is retained in the body.”
ALSO BY DR. JOHN A. HODGES | Managing phonetic complications arising in full-arch All-On-4 hybrid cases
It never ceases to amaze me that even with the established importance of chewing to our overall health, the medical insurance industry and its regulators have all but abandoned the oral health system. In my experience of working with medical insurance coverage for dental implant patients, we successfully get some form of coverage less than 20% of the time. This percentage drops below 10% when it comes to getting medical insurance coverage for full-arch rehabilitation. And in most of these cases the surgical portion is subject to coverage through medical insurance, but not the restorative portion. Although I appreciate any assistance from insurance in these cases, it is hard not to equate this lack of complete coverage to having an insurance company pay to surgically remove a patient’s bad knee and then not pay to have the new titanium knee put into place.
After the recent denial of full-arch rehabilitation for a patient of mine, I decided to try a different approach with her medical insurance company. I posed this question: Regardless of their policy toward dental implant coverage, in this patient’s case would they be financially better off paying to treat her with fixed implant-supported bridges versus not doing so and then having to pay for the future digestive complications associated with a failed oral system?
Chewing efficiency is greatly affected by how much of the teeth or bridgework in a given arch is fixed to the jawbone. Just as a person with a wooden leg would not walk as well as a person with a hinged and fitted carbon fiber prosthetic leg, a person with a tissue-supported denture will not chew as efficiently as a person with implant-supported bridges that are fused to the jawbone (figure 1).
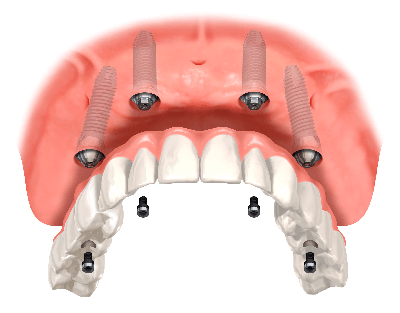
Figure 1
A person chewing with upper and lower dentures will only achieve 20% (an average of 30% for the upper denture and 10% for the lower) of the chewing efficiency of a person chewing with a full set of natural teeth, whereas a person chewing with upper and lower implant-supported bridges will achieve 90% chewing efficiency (figure 2). (2)The ability to extract additional nutrients from the food bolus can have a significantly positive impact on a patient’s overall health. Studies have tied the use of implant-supported bridges versus dentures to an increase in life expectancy of seven years. (3) To maximize a patient’s health and reduce future costs, it is important to use a fixed prosthesis versus a removable one.
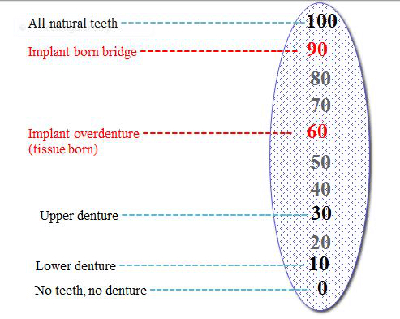
Figure 2
The long-term success rate of full-arch, implant-supported restorations is one of the best in medicine. In 2009 Dr. Paulo Malo, a world leader in full-arch, dental implant-supported bridge treatment, presented an eight-year retrospective study of 2,012 full-arch, dental implant-supported bridges treated in his practices. Of 8,048 implants that had osseointegrated after six months, only 47 were lost in the following eight years. That is an eight-year success rate of 99.18%. Reparative procedures allowed for the salvage of 100% of the bridges, so the eight-year success rate for patient function was 100%.
To put this into perspective, consider the more expensive procedure of total knee joint replacement. At an average cost of $49,500 per knee, (4) the cost to restore one leg to function is nearly double the cost to restore one dental arch to function with an implant bridge. According to Cedars Sanai, approximately 90% of replacement knee joints last 10 years, while 80% exceed 20 years. (5) This procedure is routinely covered by medical insurance, yet one could argue that although a patient’s ability to be active and quality of life are improved with a total knee replacement, the impact on overall health and possible reduction in future medical expenses are less than what would be achieved with restoring his or her oral system to near full function.
Posing the question: An excerpt from my rebuttal letter
The following is taken from a letter that I sent to a major medical insurance company for a patient whom I will call Mary.
Mary is a 42-year-old patient who had gastric bypass surgery for excessive weight five years prior to seeing me. She has suffered from multiple digestive ailments, including an inability to maintain a healthy body mass, since the surgery. Mary’s oral system is in dysfunction (figure 3), and she was referred to me by her digestive specialist in hopes of improving her ability to chew efficiently.
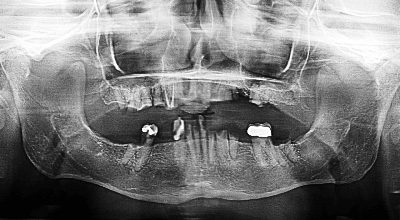
Figure 3
Mary is suffering from severe dental dysfunction. Of her 18 remaining teeth only three on her lower arch protrude through her gum tissue, and those teeth are severely decayed and functional. She is suffering from multiple chronic infections surrounding the remaining tooth fragments. On a positive note, Mary has adequate lower jaw bone to support a temporary fixed implant-supported bridge to be placed at the time of tooth extraction, and her upper jaw bone can be repaired with bone grafting at the time of tooth extraction, followed by implant placement after sufficient bone healing.
By restoring Mary’s chewing efficiency to a high level, not only can we improve her overall health and quality of life, but we can reduce the costs to your company by potentially reducing the number of medical procedures she will endure over time. Per the notes of her medical doctor, Mary has suffered multiple digestive tract complications following her gastric bypass surgery in March 2011. These complications include, but are not limited to, malnutrition, generalized abdominal pain, gastroesophageal reflux disease, esophagitis, depression, and opiate dependence.
Malnutrition
As expressed earlier, proper chewing of the food bolus can significantly improve Mary’s ability to absorb much-needed nutrients from her food. Additionally, the enzyme salivary amylase, which is contained in the saliva, initiates the breakdown of carbohydrates. Salivary amylase only works in the mouth and the esophagus. It is deactivated once it contacts stomach acids. (6) This enzyme requires prolonged chewing time in order to be effective, and Mary is currently unable to chew for any prolonged periods. Liquid carbohydrates receive insufficient salivary amylase contact time to be a substitute to chewing.
Mary’s weight dropped to 70 pounds due to malnutrition as recently as mid-2015. She required a stay in a skilled nursing facility with total parenteral nutrition (TPN) feedings. With this treatment she was able to gain 20 pounds, but since discontinuing the TPN feedings she has struggled with frequent episodes of low blood sugar.
The California Association of Health Facilities has reported that the average daily cost of a room in a skilled nursing facility is $238 per day, or $86,870 per year. In addition, TPN feedings cost $247 per day, (7) or $90,155 per year.
Cost impact per month of TPN feedings if required: $14,752
Generalized abdominal pain and opiate dependence
Chewing efficiency can impact abdominal pain. Creating a smaller food bolus with increased surface area assists acids and peristaltic contractions in the stomach to form a more uniform mixture of chime, which leads to more complete digestion. Large particles of improperly chewed food may remain undigested when they enter the intestines. This can lead to bacterial overgrowth on the undigested food (decomposition), which can lead to flatulence, bloating, abdominal pain, and even systemic infections.
It may be possible to reduce Mary’s dependence on opiates if her abdominal pain is reduced. From 2000–2007 there were 690,205,290 outpatient visits for chronic pain in the United States, costing an annual average of $17.8 billion for prescription pain medications. (8) If Mary reduces her prescription costs by $100 per month for 20 years, the cost savings would be $24,000.
Cost impact of office visits for abdominal pain and prescription opiates: Possibly $24,000 or more over 20 years
Esophagitis
In addition to the discomfort Mary experienced due to esophagitis (see opiate dependence above) her risk of a food impaction incident is greatly increased. Dr. Hin Hin Ko noted in her article, “Review of Food Bolus Management” that food impaction results from two factors. (9) The first factor is the state of the esophagus, and the second factor is the nature of the food that has been swallowed. Dr. Ko states that esophageal food impaction is a common emergency faced by gastroenterologists.
Other studies have noted:
- Food bolus impactions have underlying esophageal pathology in 88%–97% of adult patients evaluated. (10)
- 54% of adults who presented with esophageal food impactions over a three-year period had histological evidence of eosinophilic esophagitis. (11)
Dr. Ko also noted, “When these underlying esophageal conditions are present, and if food, especially meat, is chewed and swallowed precipitously, acute food impaction can occur … 10%–20% may become lodged in the esophagus or other locations in the gastrointestinal tract and may require nonoperative intervention, and 1% or less will require surgery.”
There are two primary ways that food impactions are treated nonoperatively. Patients who go to the emergency room (ER) typically have glucagons administered intravenously in hopes of getting the food impaction to spontaneously pass. This requires a CT scan of the chest to ensure that the food particle isn’t sharp. Per the National Institutes of Health, the cost of an average ER visit is $1,233 plus tests and treatment. According to New Choice Health, the average cost of a chest CT scan in Seattle is $1,935. The second means of treating a food impaction is for a gastroenterologist to perform an endoscopy to remove the food impaction or to dislodge it for digestion. New Choice Health reports that the national average cost of an endoscopy is $2,700 plus sedation and airway-management fees.
Cost impact of one food impaction episode: $3,000+
Hospitalization
Mary’s malnutrition and resultant side effects make her a very likely candidate for multiple hospital stays over the next 10 years. According to a health-care cost review by Drs. Audrey J. Weiss and Anne Elixhauser, the average cost of a hospital stay in the United States is $10,400, with an average duration of four-and-a-half days. (12)
Cost impact of hospitalization: $10,400 per 4.5-day stay
Over the next 10 years if Mary requires two months of TPN feedings in a nursing facility, two hospital stays, one food impaction to be cleared, and if she sees no reduction in her dependency on opiate medication, her medical bills likely will exceed $65,000 prior to inflation. And this projection of her treatment needs may be conservative considering the amount of care she has received in the last three years.
The cost of treating a full-arch with a dental implant-supported fixed bridge can exceed $100,000 per arch with some surgical and prosthodontic teams, but due to prices being standardized nationally by large clinics (such as Clear Choice and the Malo Clinics) that offer this service only, the price per arch is pretty consistent at $25,000–$30,000 per arch on a national level. Costs in the Pacific Northwest are consistent with this.
Even at $30,000 per arch you could see a savings of $5,000 in the first 10 years, and that savings could easily exceed $75,000 in the following 10 years.
The claim was denied again
I wish that Mary’s insurance company had seen things differently, but I wasn’t surprised. With an estimated 61,000,000 edentulous arches in the United States by 2020 (13), the thought of offering coverage must be terrifying for medical insurance companies. While understandable, I don’t have a solution to this dilemma. However, I hope the information in this article may help you draft similar arguments on behalf of your patients. Perhaps with a little luck and a lot of tenacity, we may be able to change the lives of a few fortunate people.
References
1. Rate of digestion. Science Learning Hub website. University of Waikato. http://sciencelearn.org.nz/Contexts/Digestion-Chemistry/Science-Ideas-and-Concepts/Rate-of-digestion Published July 13, 2011. Accessed August 23, 2016.
2. van der Bilt A. Human oral function: a review. Braz J Oral Sci. 2002;1(1):7–18.
3. Osterberg T, Carlsson GE, Sundh V, Steen B. Number of teeth—a predictor of mortality in the elderly? A population study in three Nordic localities. Acta Odontol Scand. 2007;65(6):335–40.
4. Greengard S. Understanding knee replacement costs: What’s on the bill? Healthline Media website. http://www.healthline.com/health/total-knee-replacement-surgery/understanding-costs#1 Published February 23, 2015. Accessed August 23, 2016.
5. Cedars-Sinai website. https://www.cedars-sinai.edu Accessed August 23, 2016.
6. Zimmerman M, Snow B. Digestion and absorption of carbohydrates. In: An Introduction to Nutrition. Creative Commons by-nc-sa 3.0 license. http://2012books.lardbucket.org/books/an-introduction-to-nutrition/index.html 2012:Chapter 4.2. http://2012books.lardbucket.org/books/an-introduction-to-nutrition/s08-02-digestion-and-absorption-of-ca.html.
7. Eisenberg JM, Glick HA, Buzby GP, Kinosian B, Williford WO. Does perioperative total parenteral nutrition reduce medical care costs? JPEN J Parenter Enteral Nutr. 1993;17(3):201–9.
8. Rasu RS, Vouthy K, Crowl AN, et al. Cost of pain medication to treat adult patients with nonmalignant chronic pain in the United States. J Manag Care Spec Pharm. 2014; 20(9): 921–8.
9. Ko HH, Enns R. Review of food bolus management. Can J Gastroenterol. 2008; 22(10):805–8.
10. Longstreth GF, Longstreth KJ, Yao JF. Esophageal food impaction: epidemiology and therapy: A retrospective observational study. Gastrointest Endosc. 2001;53(2):193–8.
11. Desai TK, Stecevic V, Chang CH, Goldstein NS, Badizadegan K, Furuta GT. Association of eosinophilic inflammation with esophageal food impaction in adults. Gastrointest Endosc. 2005;61(7):795–801.
12. Weiss AJ (Truven Health Analytics), Elixhauser A (AHRQ). Overview of Hospital Stays in the United States, 2012. HCUP Statistical Brief #180. October 2014. Agency for Healthcare Research and Quality, Rockville, MD. http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf.
13. Douglass CW, Shih A, Ostry L. Will there be a need for complete dentures in the United States in 2020? J Prosthet Dent. 2002;87(1):5–8.